Short Code 45286 Texting Details
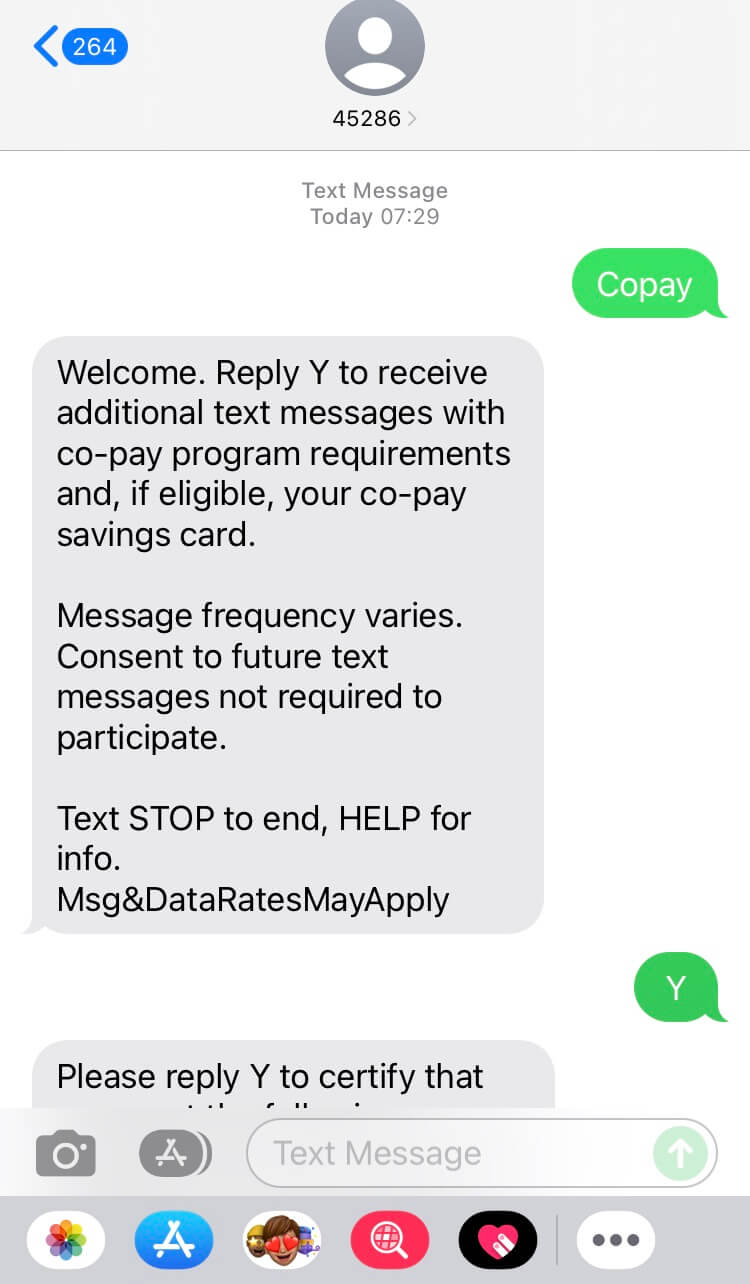
Welcome. Reply Y to receive additional text messages with co-pay program requirements and, if eligible, your co-pay savings card.
Message frequency varies. Consent to future text messages not required to participate.
Text STOP to end, HELP for info.
Msg&DataRatesMayApply
--
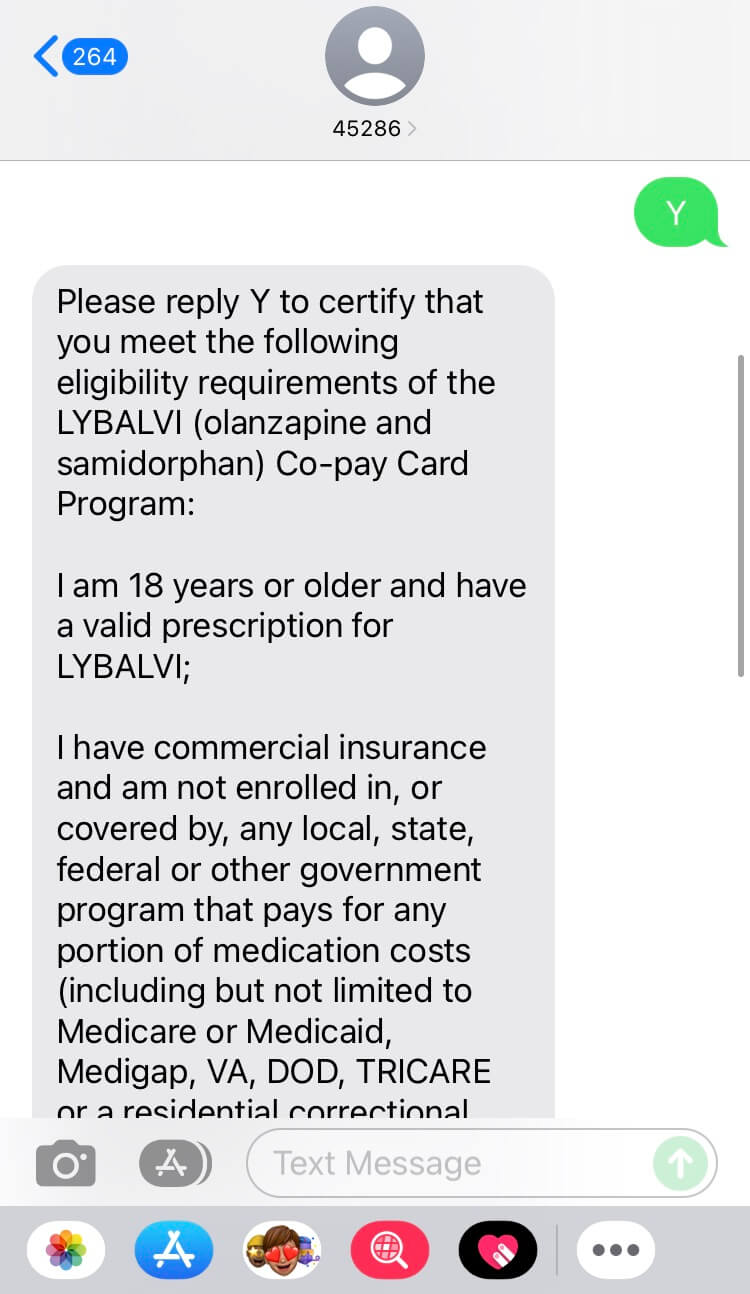
Please reply Y to certify that you meet the following eligibility requirements of the LYBALVI (olanzapine and samidorphan) Co-pay Card Program:
I am 18 years or older and have a valid prescription for LYBALVI;
I have commercial insurance and am not enrolled in, or covered by, any local, state, federal or other government program that pays for any portion of medication costs (including but not limited to Medicare or Medicaid, Medigap, VA, DOD, TRICARE or a residential correctional program); and
I have read, understand, and agree to the Program Terms and Conditions at www.LYBALVI.com/copayterms and request to participate.
See full Prescribing Information https://alkerm.es/Prescribing-Information including Boxed Warning, and Medication Guide https://alkerm.es/Lybalvi-Med-Guide for LYBALVI.
Text STOP to end, HELP for info.
--
Present the information below to your pharmacist with your prescription.
BIN: 581659
RxPCN: Loyalty
Issuer: 89563
Group: 89564785
Card ID#: 5896145277
Pharmacist Help: 1-855-820-9624 Not Health Ins. T&C apply.
To add copay card to your mobile wallet, click here: http://r.3c.com/qar. Text STOP to end.
Information and details for Short Code 45286